Life is a miracle. New life is amazing — but for various reasons, pregnancy can be murder on the low back and hips. About 50% of pregnant women experience low back or hip pain during pregnancy. And if you typically like to take a couple of ibuprofen, Aleve, or Advil for muscle or joint pain, that’s no longer an option — anti-inflammatory drugs (NSAIDs) like these can be harmful to your baby.
So what’s an expecting mom to do? Just suffer? Fortunately, the answer is no. A chiropractor can help. There are good reasons why you shouldn’t just endure pain and discomfort during pregnancy, and chiropractic care is a safe and effective way to address this problem.
Why Is Pregnancy So Painful?
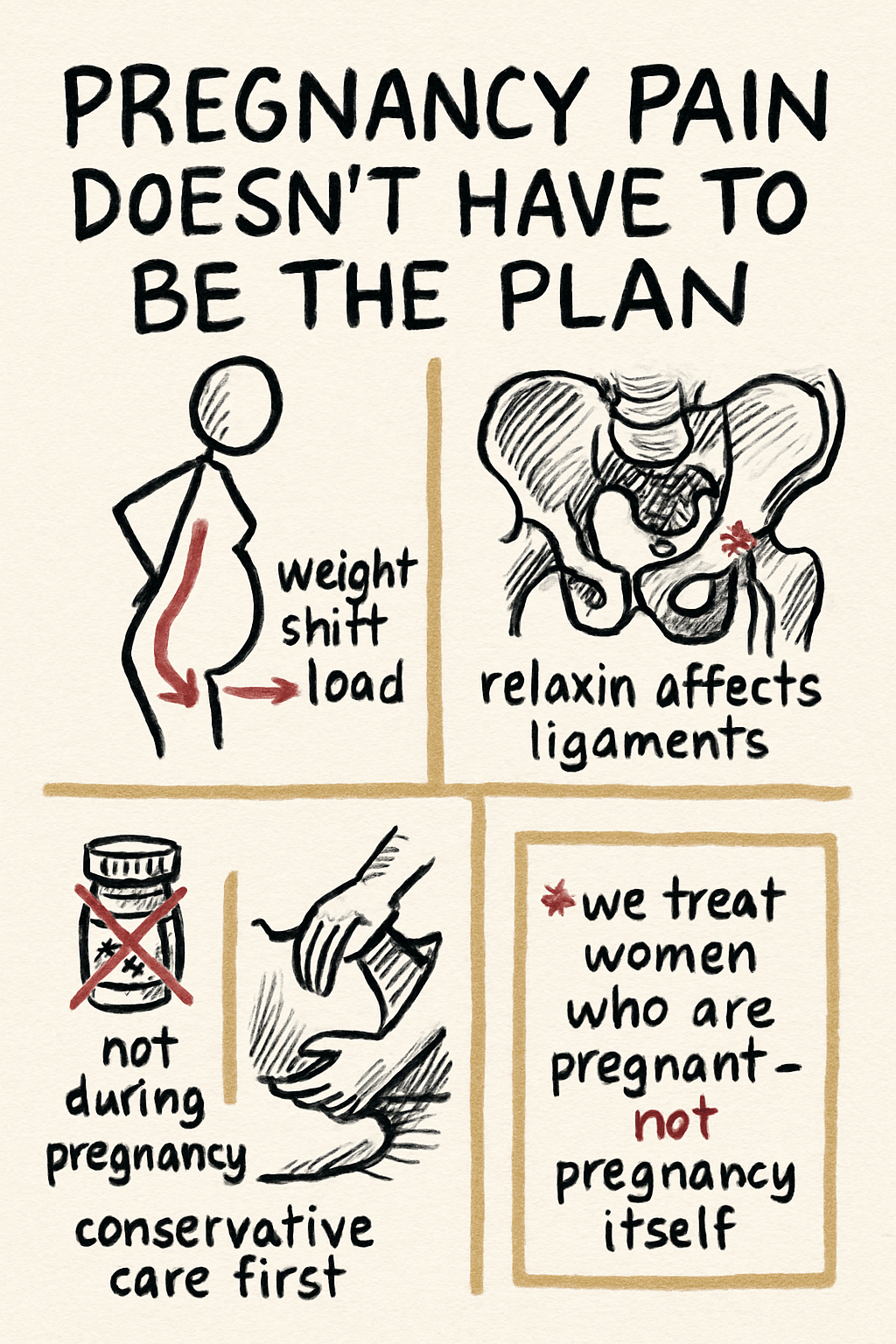
There are a number of reasons pregnancy is painful. Some of them are pretty obvious. When you look at your weight distribution, everything is shifting to the front. As your pregnancy progresses, breast and belly grow in size and cause the muscles of the back to work extra in order to keep you upright. This is one of the most common reasons for pregnant women to have muscle tension and pain during pregnancy.
In addition, there’s a hormone called relaxin that women secrete during pregnancy. The purpose of relaxin is to loosen the ligaments of the pelvis — which makes obvious sense; if the pelvis is allowed to spread, it makes delivery easier. However, relaxin works on more than just the ligaments of the pelvis. It works on every ligament in your body. Pregnant women tend to experience more ligament laxity overall, which can cause inflammation in joints, mild sprains, and increased activity in muscles that are trying to stabilize joints that are now moving more than they used to. Relaxin levels can remain elevated for several months after delivery.
Another reason for the increase in joint and muscle pain during pregnancy is a decrease in physical activity. Some women make the mistake of completely stopping exercise once they become pregnant. If your doctor says it’s safe and you were able to tolerate it well, exercise is genuinely good for pregnant women. For some that means time with the weights. For others, it’s a daily walk or run. As the pregnancy progresses, some of your ability to perform certain exercises might change — and you should always be consulting with your OB or midwife, especially if you have a high-risk pregnancy. In general, exercise can greatly improve the quality of your pregnancy by decreasing pain symptoms, reducing excess weight gain, and improving hormonal health.
The combination of a change in weight distribution, a decrease in joint stability, and a more sedentary lifestyle is a recipe for joint and muscle pain during pregnancy.
What’s Wrong With Some Pain During Pregnancy?
Just about every pregnancy involves some kind of pain — back, shoulders, neck, hips. Is there any harm in just doing nothing about it and toughing it out?
Chronic pain causes the body to secrete a hormone called cortisol. Cortisol is the main hormone associated with a stress response. It crosses the placenta — the organ that grows along with the fetus and plays the role of several organ systems. The same is true of neurotransmitters called catecholamines (adrenaline, norepinephrine, dopamine) which signal stress in our nervous system. When mom experiences stress or pain, baby is also exposed to those same stress signals.
There’s a body of research on maternal stress during pregnancy and how it may shape fetal development — particularly the developing stress-regulation systems. The data isn’t conclusive, and you shouldn’t read too much into any single finding. But it’s another reason to take pregnancy pain seriously rather than just gut it out for nine months.
There is real value in safe, effective, supportive care for expecting moms who are in pain.
So What Can a Chiropractor Do?
To be clear: chiropractors don’t treat pregnancy. We treat women who are pregnant — to help them stay comfortable, mobile, and pain-free as their bodies do something incredible.
Chiropractors are an excellent option for pregnant women who want to maintain joint and muscle health and avoid or treat the aches and pains that often come with pregnancy. Chiropractic care is a safe and effective alternative to NSAID drugs, which are not recommended during pregnancy because they can be harmful to your growing baby. Even acetaminophen (Tylenol), commonly recommended by doctors for pain control during pregnancy, has been the subject of debate over potential developmental effects — though more recent large-scale studies controlling for genetic and family factors have not found a clear causal link. The point isn’t that one medication is dangerous, and one isn’t; it’s that conservative, non-pharmacologic care should usually be the first stop for pregnancy-related musculoskeletal pain when it’s available.
One important part of our approach at Body of Health Chiropractic & Wellness Center is that we also incorporate prenatal therapeutic massage, where the chiropractor and our Licensed Massage Therapists work closely together to ensure every expectant mother gets care that’s both safe and effective.
(A bit of trivia: in the state of Oregon, chiropractors are technically licensed to deliver a baby. It’s rare these days, and we certainly don’t do it at Body of Health.)
What Does Pregnancy Chiropractic Actually Look Like?
The exam and plan format is the same as any visit — history, focused physical exam, plain-English explanation, treatment, and home exercises. What changes during pregnancy is positioning and technique:
- Side-lying setup with pregnancy pillows from mid-pregnancy onward. Standard prone (face-down) positioning isn’t comfortable past a certain point, and we don’t ask you to lie that way. If we do need to treat you while prone, we have a pregnancy pillow that allows you to lie face down comfortably and safely.
- Lower-force manipulation and joint mobilization — gentler techniques that fit pregnancy-related ligament laxity. High-velocity adjustments are used selectively when appropriate, and we always talk through what we’re going to do before we do it.
- Soft tissue therapy for the muscles that work overtime during pregnancy: hip flexors, glutes, paraspinals, mid-back, neck.
- Specific exercise and education — the right kinds of movement for the trimester you’re in, posture and lifting strategies, sleep positioning, and what to expect as things progress.
- Coordination with your OB or midwife when something needs eyes from another part of the care team.
Is Chiropractic Actually Safe for Mom and Baby?
This is the question I get most often, and it’s a fair one.
The short answer: yes, when delivered by a trained provider who adjusts their approach for pregnancy.
The longer answer involves understanding why the concern exists and what the evidence actually shows.
Why the Fetus Is Well-Protected
The uterus is a remarkably well-engineered structure for protection. The fetus is suspended in amniotic fluid, which distributes and absorbs external forces the same way a shock absorber does. The uterine wall itself is thick, muscular tissue. On top of that, layers of abdominal muscle, fat, and fascia sit between any external contact and the uterus. The forces involved in a spinal adjustment — directed at the spine and pelvis, not the abdomen — are nowhere near the threshold that would transmit meaningful force to the fetus. Trauma significant enough to threaten a pregnancy typically involves high-energy mechanisms: car accidents, falls, direct abdominal impact.
Chiropractic manipulation does not remotely approach that territory.
There’s also a practical adaptation in technique: as pregnancy progresses, we use lower-force methods, side-lying positioning, and modified contacts that reduce any mechanical load on the abdomen further. These aren’t workarounds — they’re standard prenatal practice.
What the Research Shows on Adverse Events
Chiropractic has a good safety record in the general population, and the published data on prenatal chiropractic specifically is reassuring. A 2014 systematic review found no reports of serious adverse events attributable to chiropractic care during pregnancy in the literature reviewed. Mild, short-lived soreness — the same kind you might feel after any new physical treatment — is the most commonly reported side effect. Serious complications appear to be genuinely rare, not just underreported.
That said, the evidence base here is limited by study size and design. Most of what we know comes from case series and surveys, not large randomized trials with safety as a primary endpoint. I’m not going to overstate the certainty. What I can say is that in the available literature and in practice, the risk profile looks favorable — especially when technique is adapted appropriately for each stage of pregnancy.
When Chiropractic Is NOT Appropriate During Pregnancy
There are situations where chiropractic care isn’t the right call — and a good chiropractor should be screening for these at intake and throughout care:
- Placenta previa — where the placenta partially or fully covers the cervical opening. Mechanical pelvic work is contraindicated.
- Placental abruption — premature separation of the placenta from the uterine wall. This is an obstetric emergency; it is not a chiropractic situation.
- Ectopic pregnancy — requires immediate medical management.
- Preeclampsia or other pregnancy-induced hypertension — needs OB management first. Chiropractic may still have a role in supportive care, but not as a first-line response.
- Preterm labor or risk of preterm labor — active preterm contractions are a reason to pause and consult with your OB before continuing care.
- Vaginal bleeding of unknown cause — needs obstetric evaluation before chiropractic treatment continues.
- Deep vein thrombosis — pregnancy increases clotting risk; if DVT is suspected or confirmed, manual therapy to the affected limb is contraindicated.
- High-risk pregnancy designation from your OB — not an automatic disqualifier, but it means we coordinate with your provider before proceeding.
If you have any of these conditions or your OB has flagged your pregnancy as high-risk, tell us at your first call. We’ll either coordinate with your provider or refer you to the right place. We don’t take on cases where the risk-benefit math doesn’t work.
Postpartum
Relaxin levels stay elevated for months after delivery, and many of the same mechanical loads continue postpartum — feeding positions, carrying a baby, broken sleep, return to exercise. We see postpartum patients regularly for low back, SI joint, hip, and mid-back / neck pain.
For pelvic-floor-specific work — diastasis recti rehabilitation, pelvic floor coordination and strengthening — we refer to pelvic-floor physical therapists, who do that work better than we do. The two services pair well: we handle the spine, pelvis, and hip mechanics; PFPT handles the floor.
When to Skip Us and Call Your OB Instead
Most pregnancy back, hip, and neck pain is mechanical and treatable. But some symptoms need your obstetric provider or an emergency department, not a chiropractor:
- Severe abdominal pain
- Vaginal bleeding
- Decreased fetal movement
- Sudden or severe headache, especially with vision changes or swelling (possible preeclampsia)
- Severe shortness of breath
- Signs of preterm labor
- New neurological deficit (weakness, numbness, bladder/bowel changes)
If you’re not sure whether what you’re feeling is musculoskeletal or something that needs OB attention, call us at 541·753·1287 and we’ll help you figure it out.
What This Looks Like in Corvallis and the Willamette Valley
We’ve cared for many pregnant patients across Corvallis, Albany, and the Willamette Valley over the years — first-time moms, fourth-time moms, runners, lifters, desk workers, athletes. Most see meaningful improvement within a few weeks of consistent care, and most feel substantially better through the rest of their pregnancy and into postpartum.
If you or somebody you know is pregnant and experiencing pregnancy-related low back pain or other musculoskeletal pain, give us a call. You don’t have to wait around for months to get your pain to go away. We can help.
Key Takeaways
- About half of pregnancies involve significant low back or hip pain.
- NSAIDs aren’t recommended during pregnancy, which limits the typical “just take some Advil” option.
- The fetus is well-protected by amniotic fluid, uterine muscle, and abdominal soft tissue — chiropractic forces don’t transmit meaningful risk.
- Pregnancy chiropractic care is safe and well-tolerated when delivered by a trained provider using appropriate technique. Serious adverse events are rare in the literature.
- There are real contraindications — placenta previa, abruption, active preterm labor, and others — and a good chiropractor screens for them.
- Maternal pain has effects beyond just mom — there’s reason to treat it rather than gut it out.
- Postpartum care matters too. We coordinate with pelvic-floor PTs for floor-specific work.
References
- Liddle SD, Pennick V. Interventions for Preventing and Treating Low-Back and Pelvic Pain During Pregnancy. Cochrane Database of Systematic Reviews. 2015. PubMed
- Stuge B, Veierød MB, Lærum E, Vøllestad N. The Efficacy of a Treatment Program Focusing on Specific Stabilizing Exercises for Pelvic Girdle Pain After Pregnancy. Spine. 2004. PubMed
- American College of Obstetricians and Gynecologists. Physical Activity and Exercise During Pregnancy and the Postpartum Period. ACOG Committee Opinion. 2020 (reaffirmed). ACOG
- Black E, Khor KE, Kennedy D, et al. Medication Use and Pain Management in Pregnancy. Australian Prescriber. 2019. PubMed
- Stuge B. Evidence of Stabilizing Exercises for Low Back and Pelvic Girdle Pain. Brazilian Journal of Physical Therapy. 2019. PubMed
- Glover V, O’Donnell KJ, O’Connor TG, Fisher J. Prenatal Maternal Stress, Fetal Programming, and Mechanisms Underlying Later Psychopathology — A Global Perspective. Development and Psychopathology. 2018. PubMed
- Stuber KJ, Smith DL. Chiropractic Treatment of Pregnancy-Related Low Back Pain: A Systematic Review of the Evidence. Journal of Manipulative and Physiological Therapeutics. 2008. PubMed
This information is provided for educational purposes and should not replace personalized medical advice from your obstetric provider or another qualified healthcare professional.
Made it to the end. Want the next one in your inbox?
Evidence-informed musculoskeletal content from Dr. Jason Young. One email when something new lands. Unsubscribe anytime.