Your lower back hurts when you stand up, so you assume you slept wrong, or your chair is bad, or you’re just getting older. Sometimes that’s true. Often it’s more specific than that — and the specifics matter for what you do about it.
This symptom is common: a sudden ache or sharp pain when rising from a chair, getting out of bed, or straightening after bending forward. In most cases it comes down to how the muscles, joints, and discs of the lower spine respond to movement after being held in one position. But “most cases” isn’t all cases, and knowing the difference is worth your time.
What’s Actually Happening When You Stand Up
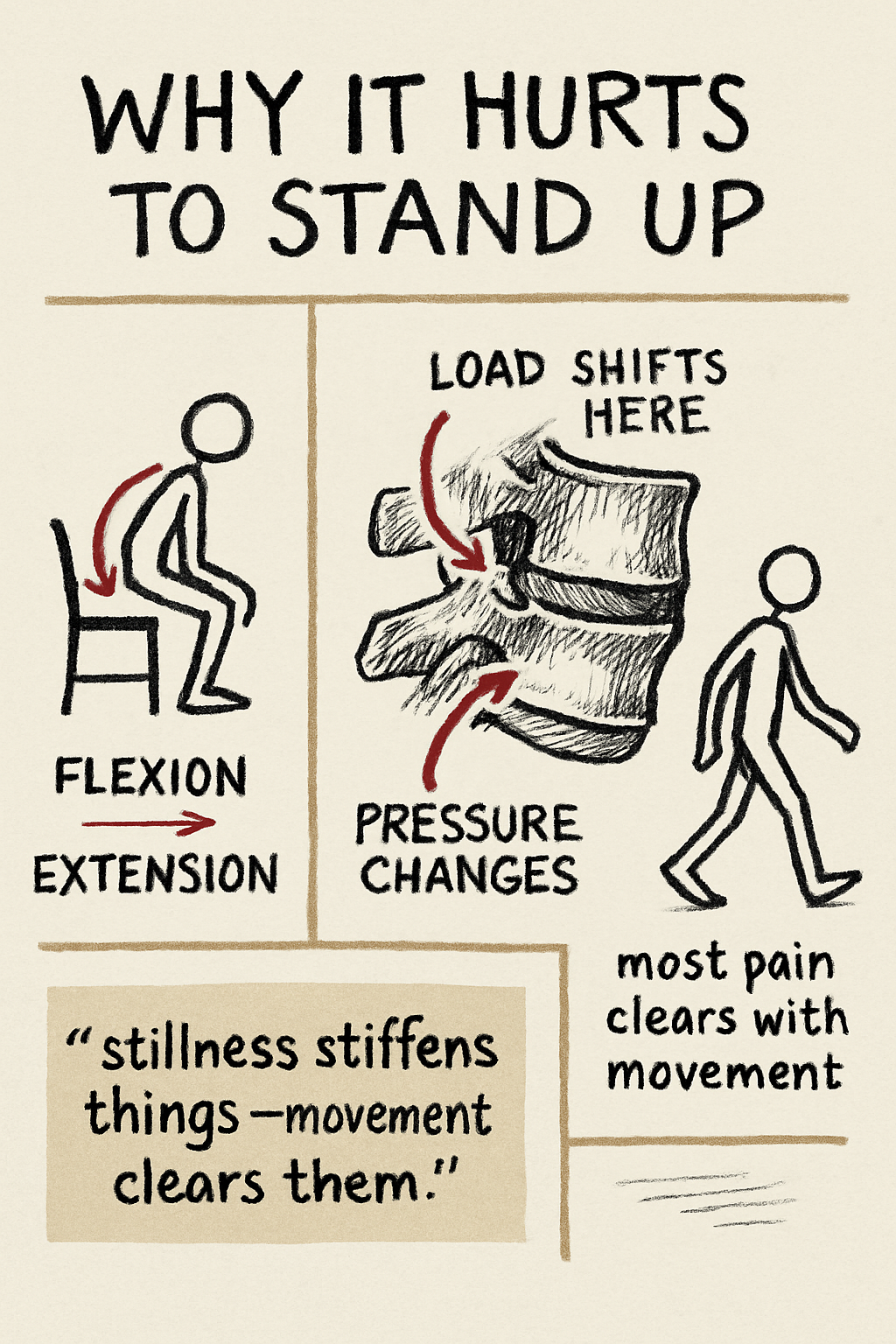
Standing up requires the spine to move from a flexed position (bent forward while sitting) into extension (upright posture). During this transition, several things happen at once: the spinal joints begin moving, the muscles around the spine activate to stabilize the body, pressure within the discs shifts, and the hips and pelvis rotate. If any of those structures are irritated or stiff, the movement can produce pain.
Muscle tightness or strain — Muscles in the lower back become tight after prolonged sitting or sleeping. When you stand, they suddenly lengthen and start working again. If they’re fatigued or stiff, that can cause a pulling sensation.
Lumbar facet joint irritation — The small joints that guide vertebral movement can become irritated from repetitive stress, arthritis, or previous injury. Standing extends the spine and can increase load on these joints. That said, facet pain can’t be diagnosed from symptoms alone and represents only a portion of mechanical low back pain cases.
Disc irritation — Pressure inside intervertebral discs changes with posture. Earlier research suggested sitting always increases disc pressure; newer data shows it depends heavily on posture — slouched sitting increases pressure, while upright supported sitting produces pressure closer to standing. If a disc is irritated, even that smaller pressure change during the sit-to-stand transition can cause discomfort.
Stiffness after prolonged stillness — Long sitting or sleeping reduces movement in the joints of the spine and hips. That stiffness can produce temporary pain that often clears after a few steps. Morning pain follows the same logic: the body stays still for hours, joints stiffen slightly, and standing up triggers a brief protest that usually settles with gentle movement.
Altered muscle coordination — Research shows that people with chronic low back pain develop changed movement patterns during sit-to-stand transitions, including altered muscle timing. These adaptations can reduce pain short-term but become problematic over time. Rehabilitation often focuses on restoring normal patterns.
Sharp Pain vs. Dull Aching Pain
The character of the pain offers some clinical signal.
Sharp pain when standing up tends to be associated with facet joint irritation, disc irritation, or sudden muscle strain.
Dull or aching pain is more often associated with muscle tightness, joint stiffness, or reduced movement after prolonged sitting.
In most cases symptoms improve after a few minutes of movement as the spine warms up. When they don’t — or when there’s a neurological component — that’s worth paying attention to.
When Lower Back Pain Might Be Something More Serious
Most movement-related lower back pain is not dangerous. However, certain symptoms require prompt medical evaluation regardless of whether they occur with sitting, standing, or anything else.
Seek care if back pain is accompanied by:
- Severe pain after trauma
- Weakness or numbness in the legs
- Loss of bowel or bladder control
- Saddle anesthesia (numbness where a saddle would touch)
- Unexplained fever or weight loss
- History of cancer
- New onset pain after age 50
- IV drug use or prolonged corticosteroid use
These red flags are uncommon but point to conditions that can’t wait.
Exercises That May Help
Gentle movement and progressive strengthening are usually the most effective long-term intervention for mechanical low back pain. Examples commonly used in rehabilitation include:
- Pelvic tilts — activate the muscles that support the spine
- Glute strengthening — reduces stress on the lumbar spine during standing and walking
- Hip mobility work — improves range of motion and reduces compensatory strain on the back
- Gentle lumbar extension movements — restore motion after prolonged sitting
Programs should be tailored to the individual and progressed gradually. Pushing through pain is rarely the answer; graded exposure usually is.
How Lower Back Pain Is Treated
Clinical guidelines recommend a biopsychosocial approach to managing low back pain, with non-pharmacological treatments first. The short version: exercise therapy produces small to moderate improvements in pain and function, manual therapy can help but works best combined with active treatment, most episodes of acute low back pain improve significantly within 4–6 weeks, and staying active generally leads to faster recovery than bed rest.
Psychological and social factors — stress, fear of movement, sleep quality, job satisfaction — also influence both development and persistence of low back pain. That’s not a dismissal of the physical component; it’s a reason to take the full picture seriously.
If you want to go deeper on common mistakes people make when managing low back pain, this episode of the PTCH Podcast covers the myths, the movement errors, and what the evidence actually suggests.
At Body of Health in Corvallis — and at our coming Albany location — care for lower back pain follows that same evidence-informed framework. Depending on the situation, that may include movement and posture evaluation, rehabilitation exercises, manual therapy to address joint stiffness or muscle tension, and education about daily movement and ergonomics. The goal is to improve how the spine moves and functions — not just chase temporary symptom relief.
Frequently Asked Questions
Why does my lower back hurt when I stand up?
The spine transitions from a bent position to an upright posture, activating muscles, shifting disc pressure, and loading the small spinal joints. If those tissues are stiff or irritated, the movement triggers temporary pain.
Why does my back hurt when I stand up after sitting?
Prolonged sitting stiffens the hips and spine and may increase disc pressure depending on posture. When you stand, the body reverses those positions quickly. Discomfort that improves after a few minutes of walking is usually mechanical.
Is lower back pain when standing up serious?
In most cases, no. It’s typically related to muscle tightness or joint stiffness. Numbness, weakness, or loss of bowel/bladder control are the exceptions — those warrant prompt evaluation.
What helps lower back pain when standing up?
Gentle movement, targeted stretching, and progressive strengthening. Staying active and gradually returning to normal activities is the consistent recommendation across clinical guidelines.
Should I see a chiropractor for lower back pain?
If pain persists, interferes with daily life, or keeps coming back, an evaluation can help identify contributing factors. Evidence-informed care typically involves movement assessment, rehabilitation exercises, manual therapy, and activity guidance.
Key Takeaways
- Lower back pain when standing up is common and usually mechanical.
- The most frequent contributors are muscle stiffness, facet joint irritation, and disc sensitivity.
- Symptoms after prolonged sitting or sleeping follow the same logic: stillness stiffens things, movement clears them.
- Gentle exercise and progressive loading are the most durable long-term intervention.
- Red flags like neurological symptoms or pain after trauma need medical evaluation, not self-management.
References
- Knezevic NN, Candido KD, Vlaeyen JWS, Van Zundert J, Cohen SP. Low Back Pain. Lancet. 2021;398(10294):78–92. PubMed
- Ghasemi Dehcheshmeh F, Nourbakhsh MR, Shafizadegan Z, et al. Pelvic and Lower Limb Kinematics in Individuals With Chronic Low Back Pain During Sit-to-Stand Function: A Cross-Sectional Study. Journal of Manipulative and Physiological Therapeutics. 2024;47(1–4):85–95. PubMed
- Wilke HJ, Neef P, Caimi M, Hoogland T, Claes LE. New In Vivo Measurements of Pressures in the Intervertebral Disc in Daily Life. Spine. 1999;24(8):755–762. PubMed
- Earwood JS, Doles NA, Russell RS. Acute Low Back Pain: Diagnosis and Management. American Family Physician. 2025;112(5):526–536. PubMed
- VA/DoD Clinical Practice Guideline. Diagnosis and Treatment of Low Back Pain. 2022. VA/DoD CPG
- Hayden JA, Ellis J, Ogilvie R, Malmivaara A, van Tulder MW. Exercise Therapy for Chronic Low Back Pain. Cochrane Database of Systematic Reviews. 2021;9:CD009790. PubMed
- Foster NE, Anema JR, Cherkin D, et al. Prevention and Treatment of Low Back Pain: Evidence, Challenges, and Promising Directions. Lancet. 2018;391(10137):2368–2383. PubMed
- Cohen SP, Raja SN. Pathogenesis, Diagnosis, and Treatment of Lumbar Zygapophysial (Facet) Joint Pain. Anesthesiology. 2007;106(3):591–614. PubMed
- Orakifar N, Shaterzadeh-Yazdi MJ, Salehi R, et al. Muscle Activity Pattern Dysfunction During Sit to Stand and Stand to Sit in the Movement System Impairment Subgroups of Low Back Pain. Archives of Physical Medicine and Rehabilitation. 2019;100(5):851–858. PubMed
Made it to the end. Want the next one in your inbox?
Evidence-informed musculoskeletal content from Dr. Jason Young. One email when something new lands. Unsubscribe anytime.