Sometimes a patient will say something like, “I have pain in my lower back, but my other problem isn’t something you can help with.”
I instantly wonder: is it something psychological? Or worse — is it cancer?!
Fortunately, it turns out it’s neither of those problems. It’s actually something I can help them with — they just have no idea that chiropractors work on things outside of back pain. They’re talking about pain in an ankle, a knee, a hip, a shoulder, or a wrist.
Chiropractors Treat the Whole Neuromusculoskeletal System
Chiropractors specialize in conditions of the neuromusculoskeletal system — that’s nerves, muscles, and bones. While most people are coming to the chiropractor for back pain, neck pain, and headaches, we can also help people who have pain in extremity joints — anything in the shoulder and arms or hips and legs.
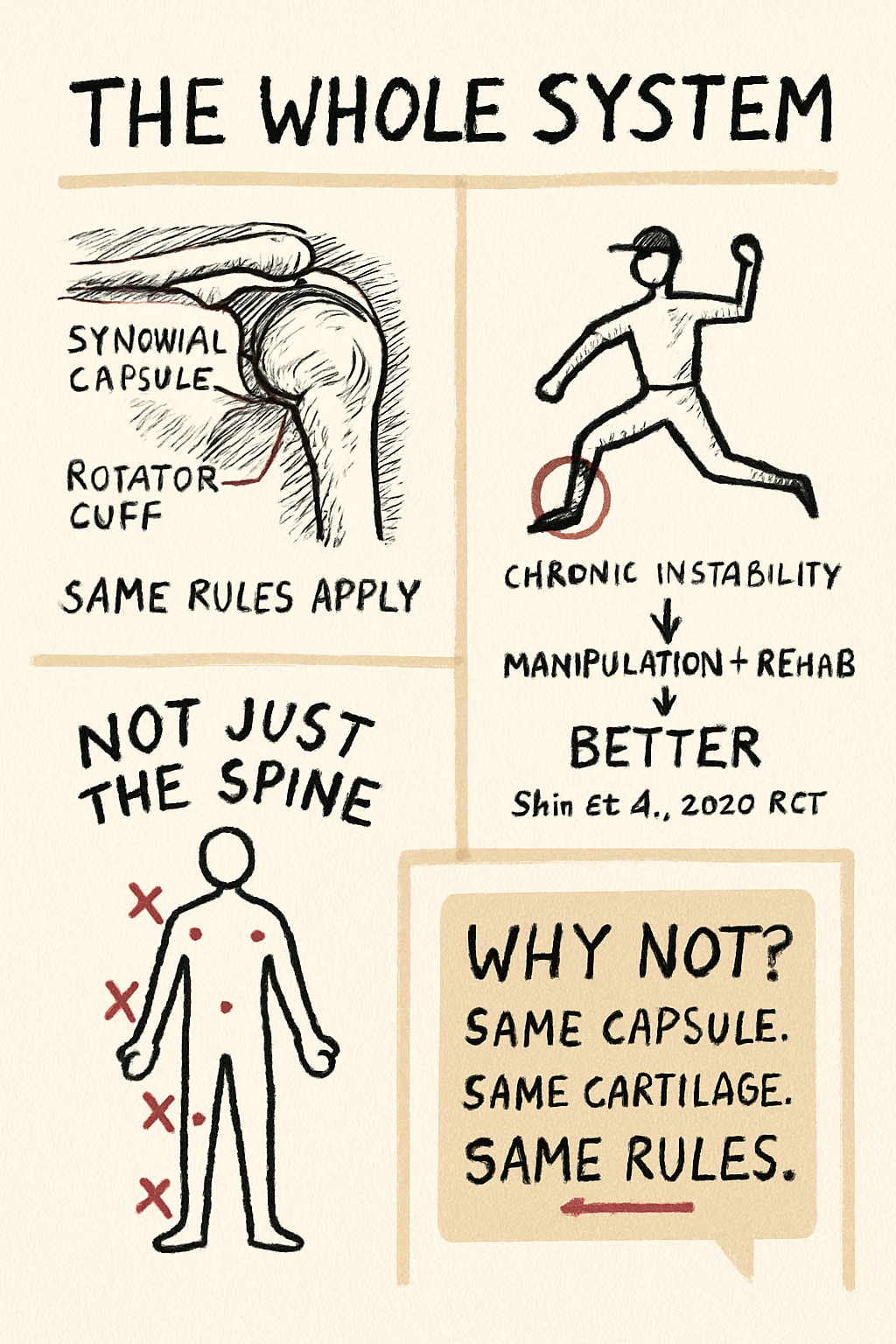
Many people wouldn’t guess that an adjustment would work on a joint outside the spine. But when you think about it, why not?
Extremity joints are surrounded by a capsule (the synovial capsule). They have cartilage inside, and fluid that lubricates the joint. They’re also surrounded by muscles, ligaments, and nerves — just like the joints of the spine. And extremity joints can become dysfunctional or stiff in much the same ways. The same way spinal manipulation can help restore normal movement to a spinal joint, extremity joint manipulation can help make an ankle, knee, hip, or wrist move better too.
A quick wrist example: A common complaint is someone who can’t do pushups because their wrist extension is stiff or painful. There are about 30 joints in the wrist and hand. Manipulation and mobilization of those joints can be remarkably helpful, and will sometimes provide immediate relief. Patients are often surprised that an issue they assumed was just “a bad wrist” actually responds to specific, targeted joint work — sometimes within the first visit.
What the Evidence Says
A 2020 randomized trial by Shin and colleagues looked at adolescent baseball players with chronic ankle instability — kids who had rolled their ankles enough times that they were left with the lingering range-of-motion deficits, proprioceptive problems, and “my ankle just doesn’t feel right” symptoms that come with repeated sprains.
Half the players received ankle manipulative therapy added to standard ankle rehabilitation. The other half got the rehab program alone. The group that received manipulation plus exercise ended up with measurably better ankle range of motion, better dynamic balance scores, and better self-reported ankle stability than the exercise-only group.
A single small trial doesn’t settle anything by itself — but it lines up with a broader pattern in the literature: combining manual therapy with active rehabilitation tends to outperform either piece alone for joint-stability and tendinopathy conditions, in athletes and non-athletes alike.
Joints We Treat and What We Do
A non-exhaustive list of extremity joints we work on:
- Shoulder — rotator cuff issues, AC joint pain, impingement-pattern complaints, frozen shoulder
- Elbow — tennis elbow (lateral epicondylitis), golfer’s elbow (medial epicondylitis), post-injury stiffness
- Wrist & hand — repetitive strain, TFCC injuries, De Quervain’s, post-fall stiffness
- Hip — gluteal tendinopathy, impingement-pattern pain, post-surgical residuals
- Knee — patellofemoral pain (“runner’s knee”), patellar tendinopathy, IT band syndrome, MCL/LCL grade I–II sprains
- Ankle & foot — chronic ankle sprains, achilles tendinopathy, plantar fasciitis
Manipulation is one tool, not the whole toolkit. For most extremity problems, the plan combines several of the following:
- Rehab exercises — graded loading is the foundation of most successful tendon and joint-stability rehab
- Radial shockwave therapy (rESWT) — for stubborn tendinopathies that haven’t responded to other care
- Myofascial release — manual soft tissue work for the muscles around the joint
- Lymphatic drainage — when post-injury swelling is part of the picture
- Taping and bracing — supportive when needed, never the whole plan
Most patients leave the first visit with hands-on treatment already started, two or three home exercises, and a clear sense of what the next few weeks should look like.
When We Refer Out
Most extremity problems respond well to conservative care, but not all of them. We refer when the exam suggests:
- Acute fracture or significant ligament rupture (orthopedic referral)
- Post-surgical restrictions still in effect (we coordinate with the surgeon)
- Joint replacement or prosthetic hardware in the joint
- Suspected systemic disease (rheumatology referral)
- Red-flag features — severe deformity, neurovascular compromise, significant swelling out of proportion to the injury
If your case is outside our scope, we’ll tell you, and we’ll point you to the right person.
What It Costs — and the Bottom Line
Most plans cover chiropractic care; we’re in-network with BCBS, PacificSource, Moda, Medicare, OHP, IHN, and VA Community Care via TriWest. Cash-pay, HSA/FSA, and a discounted time-of-service rate are also options. See our insurance page for the full breakdown →
So next time you decide your chiropractor can’t help because your joint problem isn’t just in the spine — speak up about it. You might be surprised at how much a good adjustment, paired with the right rehab plan, can do.
If you’re searching “chiropractor for knee pain in Corvallis,” “ankle adjustment in Albany,” or “shoulder pain chiropractor near me” — the answer is yes. The extremity-care page has the full picture, or just call 541·753·1287 and we’ll tell you straight whether we’re the right fit.
Key Takeaways
- Chiropractors treat the whole neuromusculoskeletal system — not just the spine.
- Extremity joints have the same kinds of capsules, cartilage, muscles, and nerves as spinal joints, and respond to manipulation and mobilization in the same way.
- Most extremity care combines manipulation with rehab exercises, soft tissue work, and sometimes shockwave therapy.
- A small RCT in adolescent baseball players with chronic ankle instability found that manipulation added to rehab outperformed rehab alone — consistent with a broader literature pattern.
- If your “other problem” is a knee, shoulder, hip, wrist, or ankle issue, mention it. We can probably help.
References
- Shin HJ, Kim SH, Jung HJ, Cho HY, Hahm SC. Manipulative Therapy Plus Ankle Therapeutic Exercises for Adolescent Baseball Players with Chronic Ankle Instability: A Single-Blinded Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2020;17(14):4997. PubMed
- Brantingham JW, Bonnefin D, Perle SM, et al. Manipulative Therapy for Lower Extremity Conditions: Update of a Literature Review. Journal of Manipulative and Physiological Therapeutics. 2012;35(2):127–166. PubMed
- Brantingham JW, Cassa TK, Bonnefin D, et al. Manipulative Therapy for Shoulder Pain and Disorders: Expansion of a Systematic Review. Journal of Manipulative and Physiological Therapeutics. 2011;34(5):314–346. PubMed
- Pribicevic M, Pollard H, Bonello R, de Luca K. A Systematic Review of Manipulative Therapy for the Treatment of Shoulder Pain. Journal of Manipulative and Physiological Therapeutics. 2010;33(9):679–689. PubMed
This information is provided for educational purposes and should not replace personalized medical advice from a qualified healthcare professional.
Made it to the end. Want the next one in your inbox?
Evidence-informed musculoskeletal content from Dr. Jason Young. One email when something new lands. Unsubscribe anytime.